Therapy vs Self-Help for Anxiety: An Evidence-Based Decision Framework for Skeptics
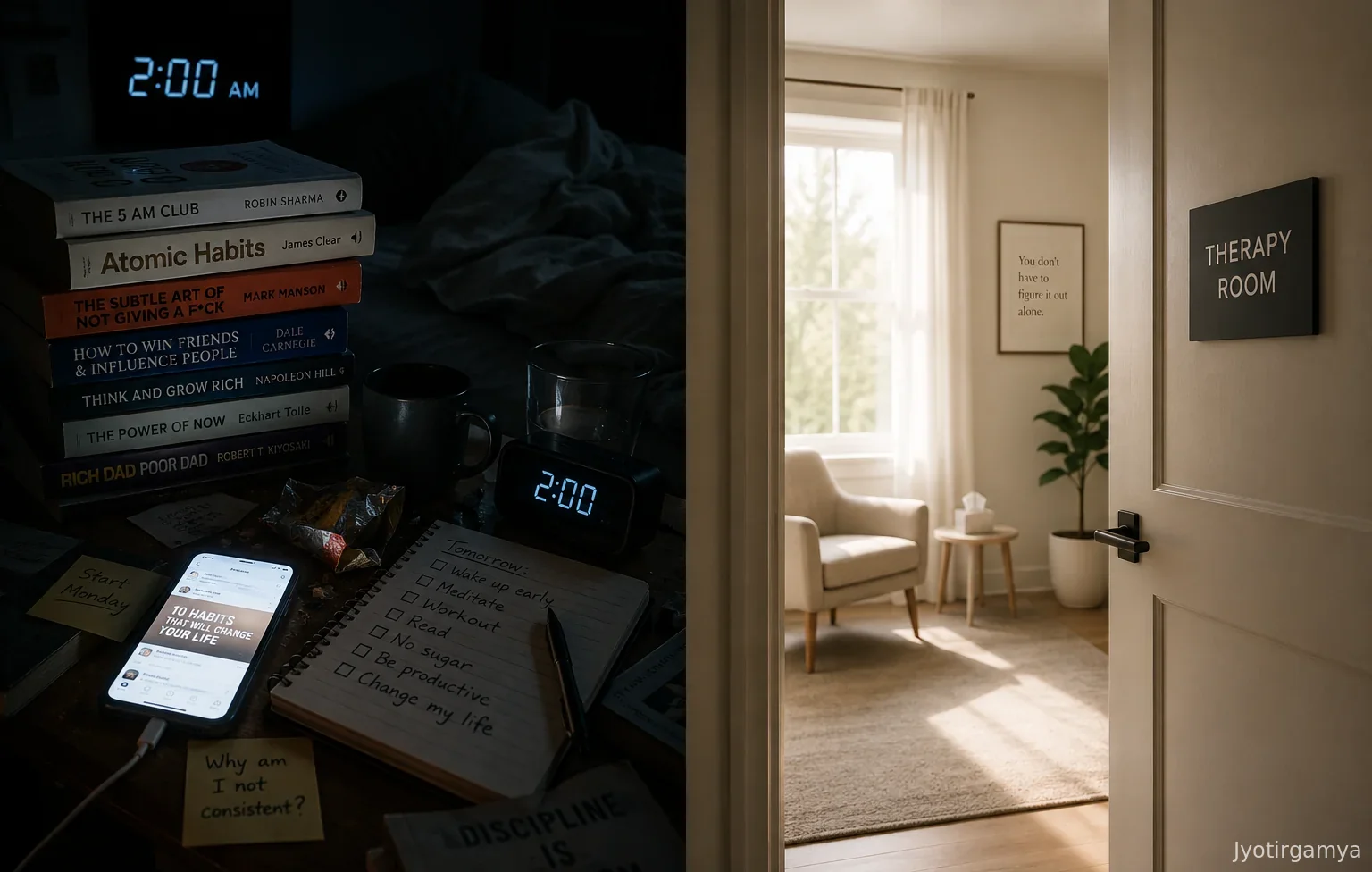
You have three unread self-help books on your nightstand, yet you are still up at 2 AM Googling symptoms to see if your anxiety is “bad enough” to justify a therapist. It is not that you lack the motivation to fix things; you simply cannot tell if you need professional intervention or just a more efficient personal system. This limbo is expensive, costing you sleep and productivity while you spin your wheels. Most high-functioning skeptics get stuck here, paralyzed by the fear of wasting money on therapy they might not need while risking failure by trying to tough it out alone. In my experience working with high-performing clients, this paralysis is often more damaging than the anxiety itself.
Research shows you do not have to guess. The Stepped Care Model, a framework validated by clinical studies, proposes starting with the least resource-intensive treatment effective for your severity level and only escalating if results plateau. We are going to apply that logic to your life. This guide breaks down a data-driven triage algorithm to help you choose between self-help and clinical treatment based on evidence, not fear.
The “Shelf of Shame”: Why Optimizing Your Treatment Is Harder Than Treating It
We need to talk about the stack of unread books on your nightstand because it is not laziness keeping those pages crisp - it is the optimization trap. You are terrified of investing twenty hours in a system that does not work, so you spend twenty hours researching systems instead. You are trying to solve the problem of execution without actually executing. This is a behavior pattern often called “hyper-reflection,” where over-analysis creates a barrier to action rather than a bridge to it. I have seen brilliant executives spend months evaluating therapy modalities only to burn out before their first session.
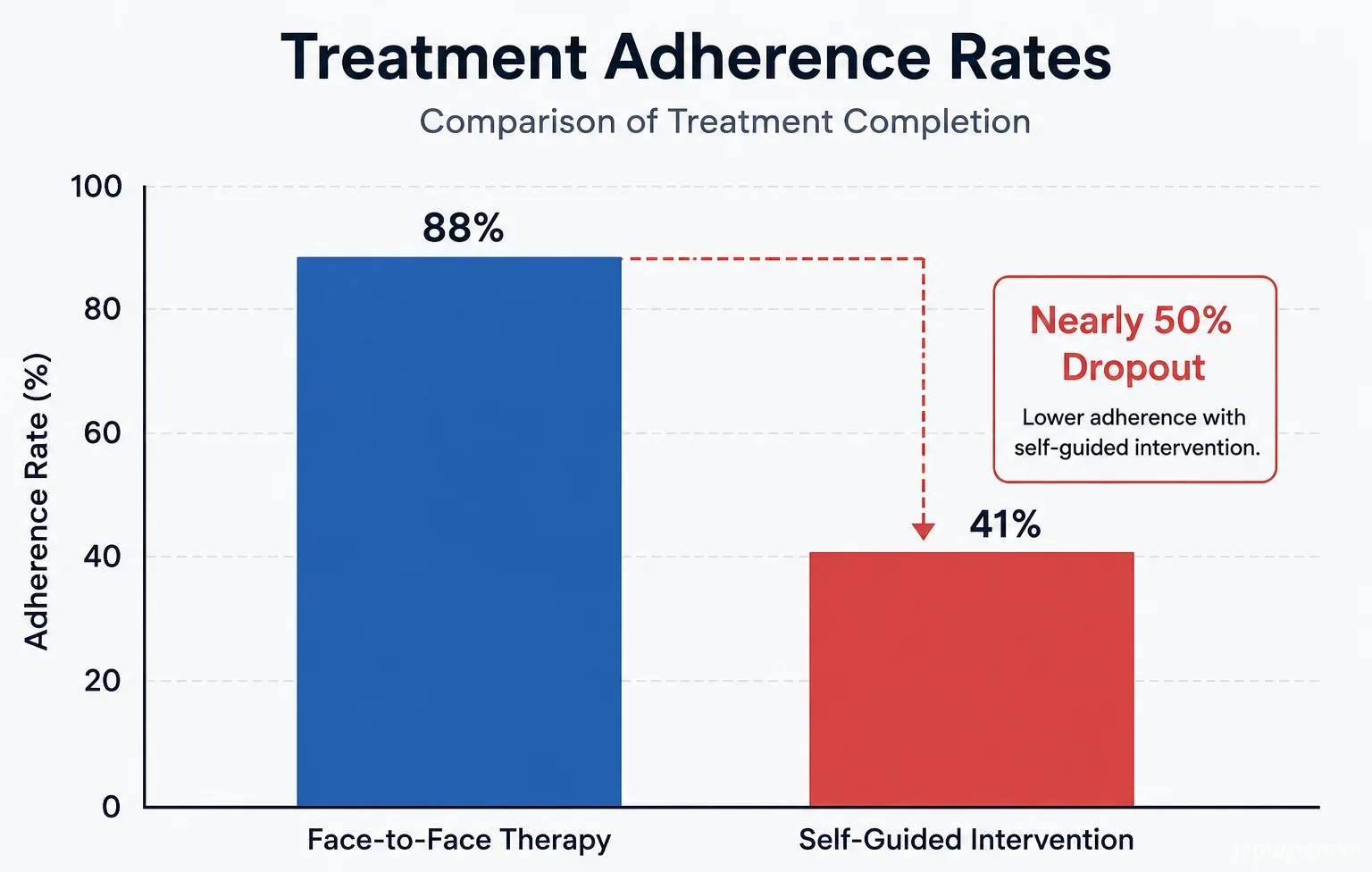
Research on bibliotherapy, or guided self-help, shows that these methods can be statistically as effective as face-to-face therapy for mild to moderate anxiety according to a meta-analysis by Cuijpers, 2010. The catch? The data only holds up if you actually do the exercises. A major review of adherence rates suggests that nearly half of users drop out of self-guided interventions before completion Christensen et al., 2009. You are failing because you are treating the selection of the treatment as the primary task, when it is actually just the admin work. The shelf of shame grows because you keep hedging your bets, looking for a guarantee that no therapist or book can offer. But you cannot optimize a process you are not currently running.
The Productivity Tax: Calculating the Hidden ROI of Indecision
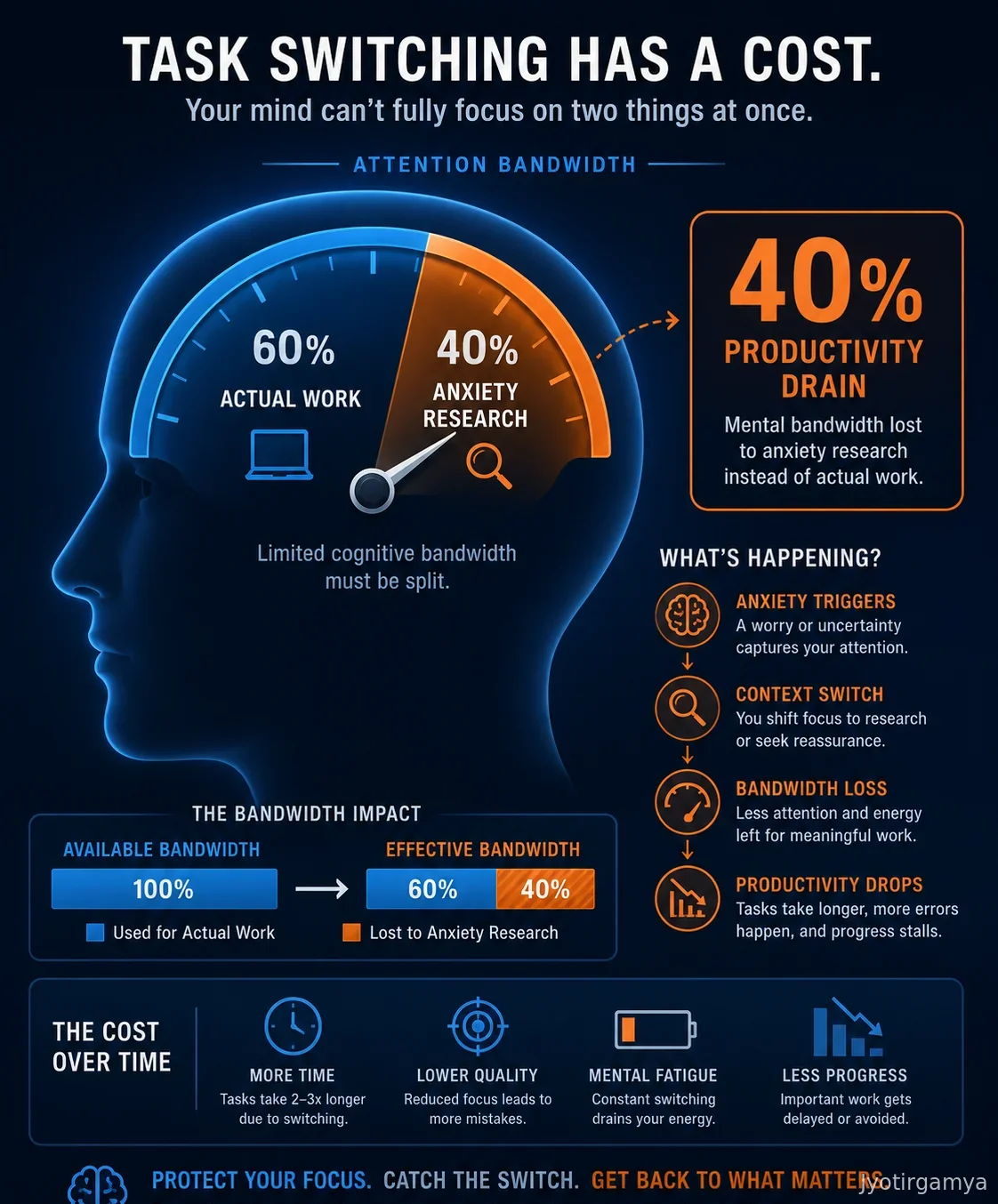
There is a hidden tax on your mental bandwidth every time you pause to calculate the ROI of a decision you haven’t made yet. Task switching costs can drain your productivity by up to 40 percent according to the American Psychological Association. You treat the search for the perfect solution as a work task, but it is actually a sophisticated avoidance mechanism. You spend hours scrolling through forums, reading reviews, and cross-referencing methodologies. You think this is due diligence. It is not. It is fear disguised as efficiency.
The cognitive load of constantly evaluating options is scientifically expensive. When you interrupt your actual work to worry about whether you are managing your anxiety correctly, you are paying double. You lose the time you spent worrying, and you lose the focus you took away from the task at hand. This hyper-reflection acts as a resource sink, stealing energy from your career and relationships to feed a loop that generates no value. A review of clinical psychology studies published in American Psychologist suggests that early intervention often yields better outcomes than waiting for the “perfect” therapeutic fit. This is largely because the factors of success are common across methods rather than unique to specific schools of thought. It is the act of showing up and doing the work that creates the change, not the specific brand of the work.
The Failure Mode: When Autonomy Becomes Avoidance
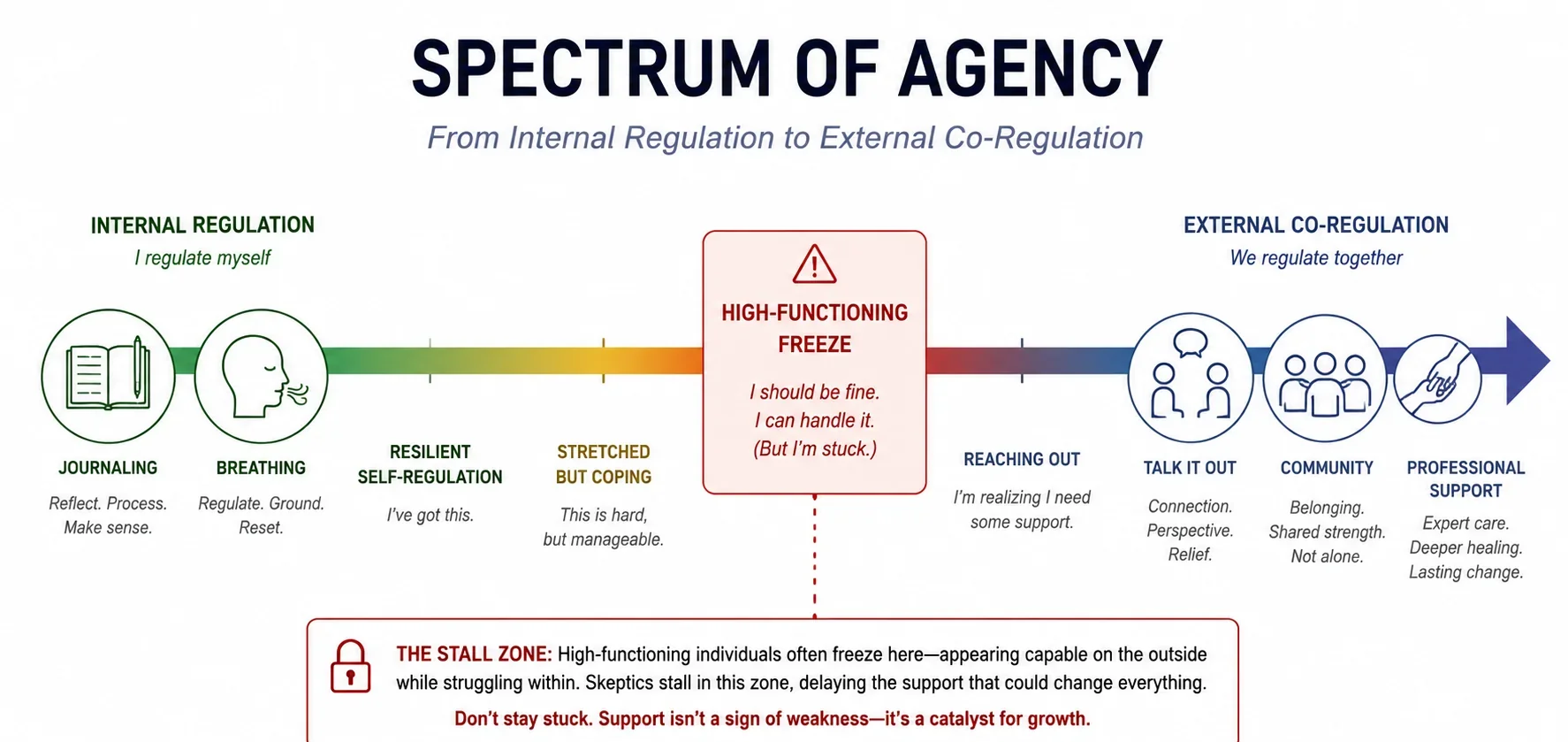
There is a subtle line between self-reliance and isolation. For the high-functioning skeptic, autonomy is a core value, but in the context of mental health, it can morph into what clinicians call the “high-functioning freeze.” You use intellectualization - reading about CBT, listening to psychology podcasts, analyzing your own triggers - as a safety behavior. It feels like progress, but it is often a way to avoid the visceral discomfort of actual exposure therapy or emotional processing.
Expert consensus suggests that unguided self-help fails most often due to a lack of an external feedback loop. When you are in the weeds of your own cognition, you lack the objectivity to catch your own distortions. This is where the “Spectrum of Agency” comes into play. Mild anxiety often responds well to internal regulation tools like journaling or breathing exercises. However, as severity increases, you typically require external co-regulation - the steady presence of another nervous system to help anchor yours. If your autonomy is preventing you from engaging in co-regulation when you need it, it has ceased to be a strength and is now a defense mechanism.
The Triage Algorithm: A Data-Driven Decision Matrix
You need a system that forces your hand, not a philosophy that fuels your hesitation, because research by Barry Schwartz et al. (2002) confirms that “maximizers” - people who obsessively seek the absolute best outcome - report significantly higher levels of regret and lower life satisfaction than “satisficers,” who accept “good enough.” You are stuck in a maximizer loop, trying to optimize a variable that does not exist yet.
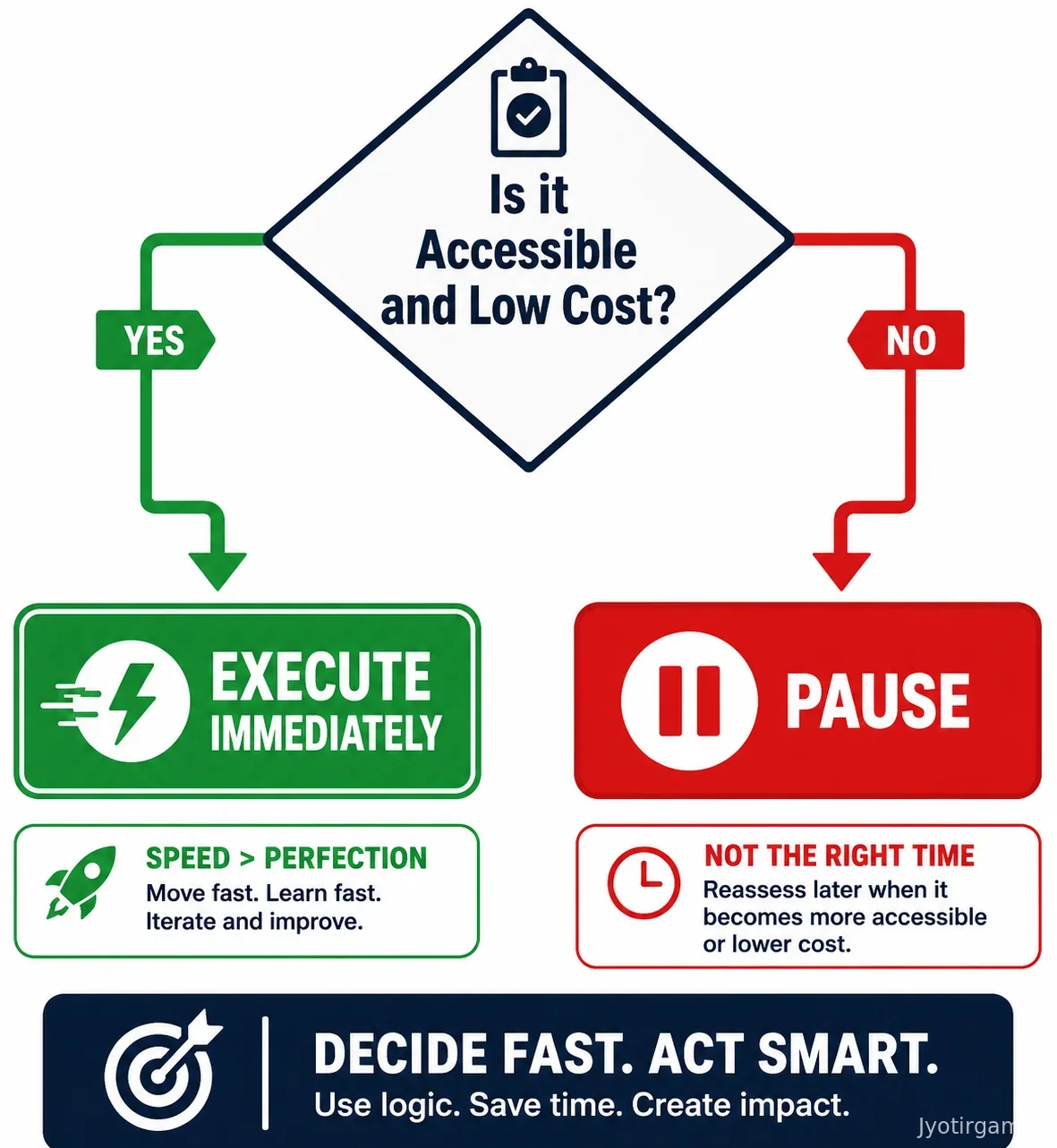
Before applying this algorithm, a necessary caveat: if you are experiencing suicidal ideation, substance abuse as a coping mechanism, or a history of severe trauma, bypass this step entirely and seek clinical care immediately. For those with mild to moderate symptoms, we use a triage approach based on Access and Cost. In emergency medicine, triage is not about curing the patient on the spot; it is about identifying who needs immediate attention to survive the crisis. You must treat your mental bandwidth with the same urgency.
If a solution is accessible to you right now and the cost of entry is low, you execute immediately. You do not ponder. You do not read fifty reviews. If you are debating between two books on anxiety, you do not spend three hours comparing Amazon ratings. You buy the one available on the shelf and start chapter one. If you can see a therapist next week for a copay, you book it. The ROI of a decent decision made today will always beat the theoretical value of a perfect decision made in three months. Speed is the only metric that matters right now. You are not looking for a lifetime partner in a self-help strategy. You are looking for a first date. Schedule it, show up, and see if the data points in the right direction.
The Middle Ground: Why Guided Self-Help Often Beats Both

For skeptics who want the efficiency of self-help with the accountability of therapy, there is a third option often overlooked: guided self-help. This hybrid approach involves working through a structured workbook or program while having brief, scheduled check-ins with a clinician. Comparative efficacy studies indicate that guided self-help often bridges the gap between unguided bibliotherapy and full face-to-face therapy, offering remission rates significantly higher than going it alone.
From a pragmatic standpoint, this is your sweet spot. It limits the financial exposure while providing the external feedback loop required to break the “optimization trap.” You are not left to your own devices to interpret your progress, nor are you paying for hourly deep-dives you might not need yet. It creates a forcing function. You have to do the work because you know someone will ask you about it on Tuesday.
Stop Researching, Start Triage
The cost of your current limbo is far higher than the cost of a “wrong” choice, because at least a wrong choice generates data you can use. You have the framework now. The hesitation has to end. The Stepped Care Model is not about fixing yourself perfectly in one go. It is about moving the needle. Pick the accessible option today. Commit to the process for thirty days. If you hit a plateau, you step up the care. But you have to take the first step to find the plateau. Close the research tabs and open the book. The only way to optimize your life is to actually live it.
Frequently Asked Questions
Guided self-help can be statistically as effective as face-to-face therapy for mild to moderate anxiety. However, nearly half of users drop out of unguided interventions before completion due to a lack of accountability.
Use the Stepped Care Model to triage your symptoms by starting with the least resource-intensive option. If self-help is accessible and low-cost, execute immediately and only seek a therapist if your progress plateaus.
Self-help fails when over-analysis replaces execution, creating a barrier known as 'hyper-reflection.' Without an external feedback loop or co-regulation, it is difficult to maintain objectivity and adherence to the program.
 Conquer Anxiety with Hypnotherapy
Conquer Anxiety with Hypnotherapy
 Do I Need Therapy for ADHD? A Data-Driven Decision Framework
Do I Need Therapy for ADHD? A Data-Driven Decision Framework
 7 Proven Strategies to Turn Fear into Fuel
7 Proven Strategies to Turn Fear into Fuel
 CBT vs. ACT vs. DBT for Anxiety: An Evidence-Based Decision Framework
CBT vs. ACT vs. DBT for Anxiety: An Evidence-Based Decision Framework
 The Architecture of Relief: A Data-Driven Framework for Choosing Your Anxiety Therapy
The Architecture of Relief: A Data-Driven Framework for Choosing Your Anxiety Therapy
 Therapy vs Self-Help for Anxiety: An Evidence-Based Decision Matrix for Skeptics
Therapy vs Self-Help for Anxiety: An Evidence-Based Decision Matrix for Skeptics